This is an online E logbook to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from an available global online community of experts to solve those patients clinical problems with collective current best evidence-based inputs. This e-log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box are welcome.
I’ve been given this case to solve in an attempt to understand the topic of “patient
clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan.
Following is the view of my case :
Date of admission : 5-9-2022
Chief complaints :
A 15-year-old-male patient came to the casualty with the cheif complaints of fever 5 days back
Burning micturition since 4-5 days
Difficulty in micturition since 4-5 dayz
History of present illness : patient was apparently asymtomatic 10 days back ,then developed
H/o Fever-
Onset - insidious
Duration- for 3 days
Type - intermittant ,low grade
It was relieving on taking medications .
Not Associated with chills and rigors.
Not Associated with generalised body aches and weakness
Diurnal variation absent
No increased temperature at night
After his fever got subsided, he had
H/0 burning micturition - since 4-5 days
H/0 pain while urinating , and poor stream.
10 days back, he went to a local hospital at nalgonda for fever ,he got treated for it and his fever subsided.
He got his reports done which showed,
Widal test- positive
...later
him came to our hospital because his parents didnt like that hospital.
Daily routine- wakes up at 8:00 am
Drinks milk at 9:00 am
Goes to college-he is studying intermediate
Lunch at 12:00 pm
Returns from college at 4:00 pm
Takes rest, goes to roam with his friends .
Sleeps at 10:00 pm
History of past illness :
Not a known case of,
diabetes, epilepsy, CAD, asthma, thyroid.
Personal history :
Diet - mixed
Appetite - normal
sleep - adequate
Bowel and Bladder movements -burning micturition
Addictions - no
No known allergies
Drug history :
No significant drug history
Family history :
No significant family history
General examination :
Patient is conscious ,coherent ,cooperative and was well oriented to time ,place and person
at the time of examination
SHe is examined in a well lit room, with consent taken.
SHe is moderately built and well nourished.
Pallor - present
Icterus - absent
Cyanosis - absent
Clubbing - absent
lymphadenopathy - absent
Pedal edema - absent
Systemic examination :
CVS : S1 and S2 heart sounds heard
NO murmurs and thrills
RESPIRATORY SYSTEM : Bilateral air entry present position of trachea - centrall
Vesicular breathsounds heard
CNS : intact
ABDOMEN :
Soft non tender
Splenomegaly present
Bowel sounds heard
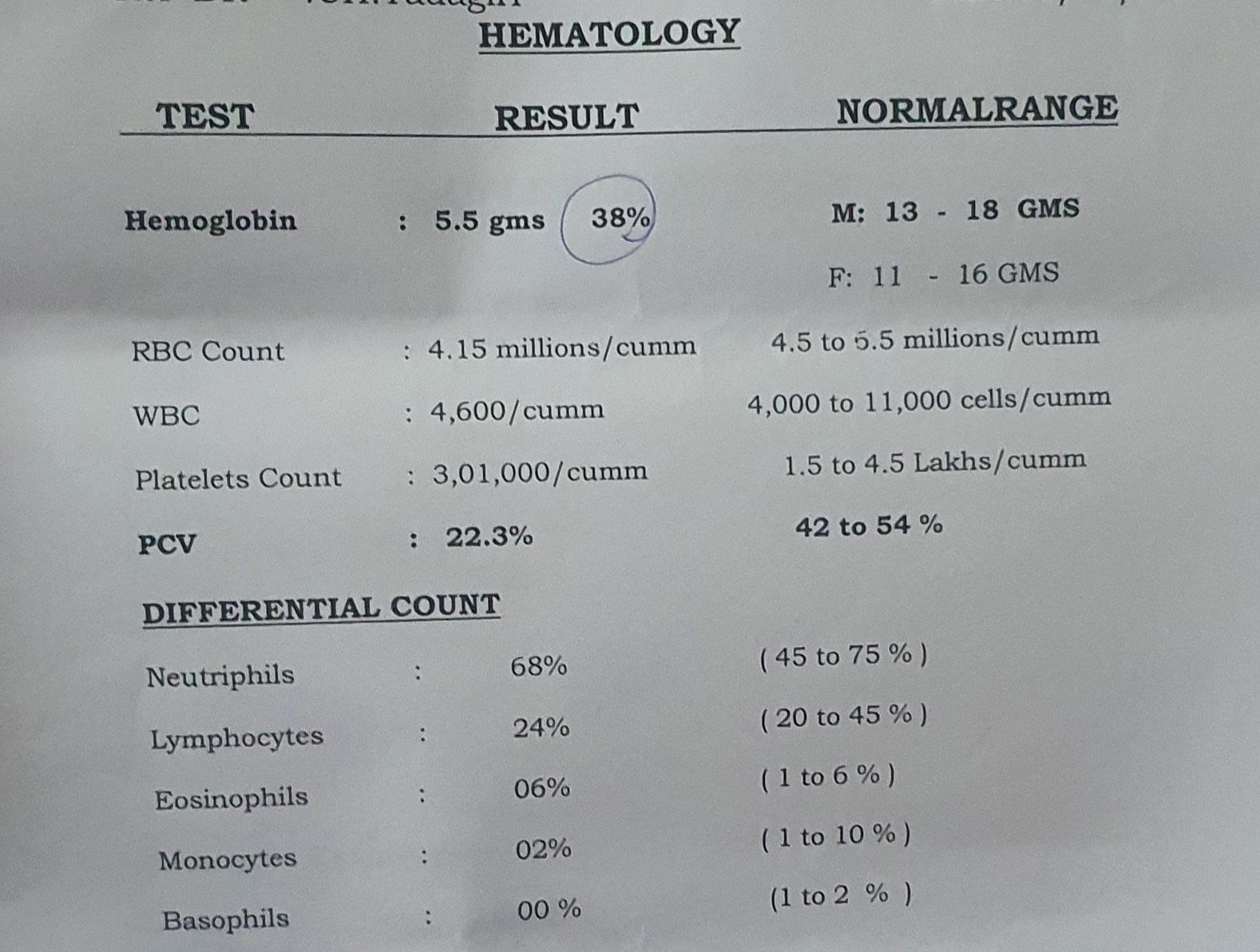
Investigations:
On day 1 (5-9-22)
On day 2 (6-9-22)
IRON DEFICIENCY ANAEMIA(SECONDARY TO ?NUTRITIONAL CAUSE) UTI(RECOVERED) SECONDARY TO PHIMOSIS
WITH DELAYED PUBERTY
Treatment:
On day 1 (5-9-22)
1.Tab DOLO 650mg PO SOS
2.Tab. Zincovit PO OD
On day 2 (6-9-22)
1. Tab. DOLO 650 mg PO SOS
2. INJ. Optineuron 1amp in 100ml NS/ IV/OD
3.SYP. Citralka 15ml in glass of water PO/TID
On day 3 (7-9-22)
Tab. DOLO 650 mg PO SOS
2. INJ. Optineuron 1amp in 100ml NS/ IV/OD
3.SYP. Citralka 15ml in glass of water PO/TID
On day 4 (8-9-22)
Tab. DOLO 650 mg PO SOS
2. INJ. Optineuron 1amp in 100ml NS/ IV/OD
3.SYP. Citralka 15a ml in glass of water PO/TID
Discharge summery
Date:9-SEP-2022
Ward:MEDICAL WARD
Unit: 1
Diagnosis
IRON DEFICIENCY ANAEMIA(SECONDARY TO ?NUTRITIONAL CAUSE) UTI(RECOVERED) SECONDARY TO PHIMOSIS
WITH DELAYED PUBERTY
Chief complaints :
A 15-year-old-male patient came to the casualty with the cheif complaints of fever 5 days back
Burning micturition since 4-5 days
Difficulty in micturition since 4-5 dayz
History of present illness : patient was apparently asymtomatic 10 days back ,then developed
H/o Fever-
Onset - insidious
Duration- for 3 days
Type - intermittant ,low grade
It was relieving on taking medications .
Not Associated with chills and rigors.
Not Associated with generalised body aches and weakness
Diurnal variation absent
No increased temperature at night
After his fever got subsided, he had
H/0 burning micturition - since 4-5 days
H/0 pain while urinating , and poor stream.
10 days back, he went to a local hospital at nalgonda for fever ,he got treated for it and his fever subsided.
Daily routine- wakes up at 8:00 am
Drinks milk at 9:00 am
Goes to college-he is studying intermediate
Lunch at 12:00 pm
Returns from college at 4:00 pm
Takes rest, goes to roam with his friends .
Sleeps at 10:00 pm
History of past illness :
Not a known case of,
diabetes, epilepsy, CAD, asthma, thyroid.
Personal history :
Diet - mixed
Appetite - normal
sleep - adequate
Bowel and Bladder movements -burning micturition
Addictions - no
No known allergies
Drug history :
No significant drug history
Family history :
No significant family history
General examination :
Patient is conscious ,coherent ,cooperative and was well oriented to time ,place and person
at the time of examination
SHe is examined in a well lit room, with consent taken.
SHe is moderately built and well nourished.
Pallor - present
Icterus - absent
Cyanosis - absent
Clubbing - absent
lymphadenopathy - absent
Pedal edema - absent
Systemic examination :
CVS : S1 and S2 heart sounds heard
NO murmurs and thrills
RESPIRATORY SYSTEM : Bilateral air entry present , position of trachea - centrall
Vesicular breathsounds heard
CNS : intact
ABDOMEN :
Soft non tender
Splenomegaly present
Bowel sounds heard
Investigations:
| | | COMPLETE URINE EXAMINATION (CUE) 05-09-2022 05:50:PM | | COLOUR | Pale yellow | | | APPEARANCE | Clear | | | REACTION | Acidic | | | SP.GRAVITY | 1.010 | | | ALBUMIN | Nil | | | SUGAR | Nil | | | BILE SALTS | Nil | | | BILE PIGMENTS | Nil | | | PUS CELLS | 2-3 | | | EPITHELIAL CELLS | 1-2 | | | RED BLOOD CELLS | Nil | | | CRYSTALS | Nil | | | CASTS | Nil | | | AMORPHOUS DEPOSITS | Absent | | | OTHERS | Nil | |
| | HBsAg-RAPID 05-09-2022 05:50:PM | Negative | |
| | Anti HCV Antibodies - RAPID 05-09-2022 05:50:PM | Non Reactive | |
| | LIVER FUNCTION TEST (LFT) 05-09-2022 05:50:PM | | Total Bilurubin | 0.69 mg/dl | 1-0 mg/dl | | Direct Bilurubin | 0.10 mg/dl | 0.2-0.0 mg/dl | | SGOT(AST) | 33 IU/L | 35-0 IU/L | | SGPT(ALT) | 15 IU/L | 45-0 IU/L | | ALKALINE PHOSPHATE | 200 IU/L | 369-54 IU/L | | TOTAL PROTEINS | 7.4 gm/dl | 8-6 gm/dl | | ALBUMIN | 3.9 gm/dl | 4.5-3.2 gm/dl | | A/G RATIO | 1.09 | |
| | RFT 05-09-2022 05:50:PM | | UREA | 11 mg/dl | 42-12 mg/dl | | CREATININE | 0.5 mg/dl | 1-0.5 mg/dl | | URIC ACID | 3.7 mg/dl | 7.2-3.5 mg/dl | | CALCIUM | 9.7 mg/dl | 10.2-8.6 mg/dl | | PHOSPHOROUS | 4.4 mg/dl | 4.5-2.5 mg/dl | | SODIUM | 139 mEq/L | 145-136 mEq/L | | POTASSIUM | 4.6 mEq/L | 5.1-3.5 mEq/L | | CHLORIDE | 98 mEq/L | 98-107 mEq/L |
| | COMPLETE URINE EXAMINATION (CUE) 06-09-2022 05:22:PM | | COLOUR | Pale yellow | | | APPEARANCE | Clear | | | REACTION | Acidic | | | SP.GRAVITY | 1.010 | | | ALBUMIN | Nil | | | SUGAR | Nil | | | BILE SALTS | Nil | | | BILE PIGMENTS | Nil | | | PUS CELLS | 2-4 | | | EPITHELIAL CELLS | 2-3 | | | RED BLOOD CELLS | Nil | | | CRYSTALS | Nil | | | CASTS | Nil | | | AMORPHOUS DEPOSITS | Absent | | | OTHERS | Nil | |
| |
|
|
| | | COMPLETE URINE EXAMINATION (CUE) 05-09-2022 05:50:PM | | COLOUR | Pale yellow | | | APPEARANCE | Clear | | | REACTION | Acidic | | | SP.GRAVITY | 1.010 | | | ALBUMIN | Nil | | | SUGAR | Nil | | | BILE SALTS | Nil | | | BILE PIGMENTS | Nil | | | PUS CELLS | 2-3 | | | EPITHELIAL CELLS | 1-2 | | | RED BLOOD CELLS | Nil | | | CRYSTALS | Nil | | | CASTS | Nil | | | AMORPHOUS DEPOSITS | Absent | | | OTHERS | Nil | |
| | HBsAg-RAPID 05-09-2022 05:50:PM | Negative | |
| | Anti HCV Antibodies - RAPID 05-09-2022 05:50:PM | Non Reactive | |
| | LIVER FUNCTION TEST (LFT) 05-09-2022 05:50:PM | | Total Bilurubin | 0.69 mg/dl | 1-0 mg/dl | | Direct Bilurubin | 0.10 mg/dl | 0.2-0.0 mg/dl | | SGOT(AST) | 33 IU/L | 35-0 IU/L | | SGPT(ALT) | 15 IU/L | 45-0 IU/L | | ALKALINE PHOSPHATE | 200 IU/L | 369-54 IU/L | | TOTAL PROTEINS | 7.4 gm/dl | 8-6 gm/dl | | ALBUMIN | 3.9 gm/dl | 4.5-3.2 gm/dl | | A/G RATIO | 1.09 | |
| | RFT 05-09-2022 05:50:PM | | UREA | 11 mg/dl | 42-12 mg/dl | | CREATININE | 0.5 mg/dl | 1-0.5 mg/dl | | URIC ACID | 3.7 mg/dl | 7.2-3.5 mg/dl | | CALCIUM | 9.7 mg/dl | 10.2-8.6 mg/dl | | PHOSPHOROUS | 4.4 mg/dl | 4.5-2.5 mg/dl | | SODIUM | 139 mEq/L | 145-136 mEq/L | | POTASSIUM | 4.6 mEq/L | 5.1-3.5 mEq/L | | CHLORIDE | 98 mEq/L | 98-107 mEq/L |
| | COMPLETE URINE EXAMINATION (CUE) 06-09-2022 05:22:PM | | COLOUR | Pale yellow | | | APPEARANCE | Clear | | | REACTION | Acidic | | | SP.GRAVITY | 1.010 | | | ALBUMIN | Nil | | | SUGAR | Nil | | | BILE SALTS | Nil | | | BILE PIGMENTS | Nil | | | PUS CELLS | 2-4 | | | EPITHELIAL CELLS | 2-3 | | | RED BLOOD CELLS | Nil | | | CRYSTALS | Nil | | | CASTS | Nil | | | AMORPHOUS DEPOSITS | Absent | | | OTHERS | Nil | |
| |
|
|
| Treatment Given(Enter only Generic Name) |
1. Tab. OROFERXT twice daily 8am. 8pm ( before food) 2. Tab. limcee twice daily 8am. 8pm 3. Syp. Dexorange. 10ml thrice daily 8am. 2pm. 8pm | |
|
|
|
Followup:
Review to opd after 15 days with hemoglobin and reticount
IN CASE OF ANY EMERGENCY IMMEDIATELY CONTACT YOUR CONSULTANT DOCTOR OR ATTEND EMERGENCY DEPARTMENT.
AVOID SELF MEDICATION WITHOUT DOCTORS ADVICE,DONOT MISS MEDICATIONS. Patient/Attendent Declaration : - The medicines prescribed and the advice regarding preventive aspects of care ,when and how to obtain urgent care have been explained to me in my own language
SIGNATURE OF PATIENT /ATTENDER
SIGNATURE OF PG/INTERNEE
SIGNATURE OF ADMINISTRATOR
SIGNATURE OF FACULTY





















Comments
Post a Comment